Arteriovenous Fistula (AVF) and Arteriovenous Graft
(AVG) Placement are surgical procedures used to create access
points in the circulatory system for patients who require hemodialysis, a
medical treatment for individuals with kidney failure or end-stage renal
disease (ESRD). These access points allow for efficient removal and return of
blood during hemodialysis treatments. Both AVFs and AVGs are used to facilitate
the connection between the patient and the hemodialysis machine.
Here's an overview of these procedures:
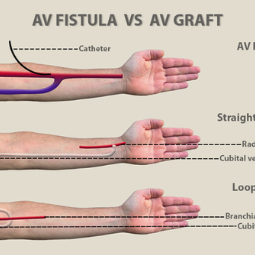
Arteriovenous Fistula (AVF) Placement:
Purpose: An AVF is
a direct connection between an artery and a vein, typically created in the
patient's forearm. The purpose of an AVF is to provide a natural, long-lasting
access point for hemodialysis. The connection allows for high blood flow,
making it easier for the dialysis machine to filter the blood efficiently.
Procedure: During
AVF placement, a surgeon typically locates a suitable artery and vein in the
forearm. A connection is then surgically created, often by joining the artery
and vein or by sewing a segment of vein into the side of the artery. This
connection enlarges the vein over time, making it more suitable for repeated
needle insertions.
Maturation: After AVF
placement, it takes some time for the fistula to mature and become usable for
hemodialysis. Maturation typically takes several weeks to a few months.
Arteriovenous Graft (AVG) Placement:
Purpose: An AVG is
a synthetic tube (graft) implanted under the skin, connecting an artery and a
vein. The purpose of an AVG is to provide a suitable access point for
hemodialysis when a patient's veins are not suitable for AVF creation or have
previously failed.
Procedure: During
AVG placement, a surgeon typically inserts a synthetic graft under the skin,
connecting an artery and a vein. The graft serves as an artificial access point
for hemodialysis, allowing repeated needle insertions. AVGs can be used sooner
than AVFs, often within a few weeks after placement.
Maintenance: AVGs may
require more regular monitoring and maintenance compared to AVFs, as they can
be prone to complications such as infection or clotting.
Both AVFs and AVGs are used to provide efficient and reliable access for
hemodialysis treatments, allowing patients with ESRD to receive life-sustaining
dialysis. The choice between AVF and AVG placement depends on various factors,
including the patient's overall health, vascular condition, and the
availability of suitable veins for an AVF. The specific procedure and site are
determined by a vascular surgeon or an interventional radiologist in
collaboration with the patient's healthcare team. Regular care and maintenance
are essential to ensure the longevity and effectiveness of these access points.



.png)